
Organ-on-chip models vs. ANIMAL MODELS [1, 2]
| |
+ |
|
– |
|

Organ-on-chip models vs. EX VIVO CULTURES (e.g., biopsy samples) [3, 4]
| |
+ |
|
– |
|
Organ-on-chip models vs. 2D CELL CULTURES [3, 4]
| |
+ |
|
– |
|
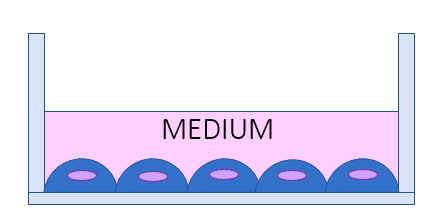
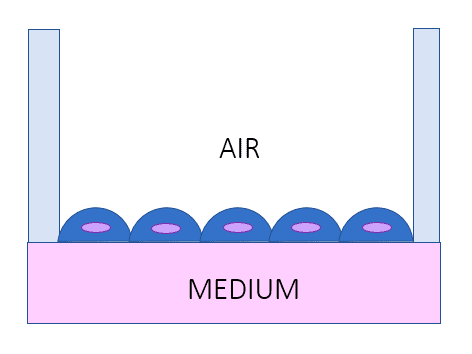
Organ-on-chip models vs. AIR-LIQUID INTERFACE LUNG MODEL [1, 5]
| |
+ |
|
– |
|
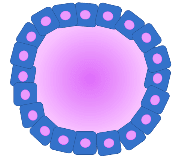
Organ-on-chip models vs. ORGANOIDS [6, 7]
| |
+ |
|
– |
|
Organ-on-chip models vs. TISSUE ENGINEERING (1)
Artificial constructs [8-10] | |
+ |
|
– |
|

Organ-on-chip models vs. TISSUE ENGINEERING (2)
Biological (decellularized) constructs [8–10] | |
+ |
|
– |
|

