|
Authors: *corresponding authour: Elvesys SAS, 172 Rue de Charonne |
 |
Microfluidic reviews
Recent research breakthroughs in lung-on-chip technology

Development of new therapeutic drugs is decreasing while research costs are rising. A study from the Tufts Center for the Study of Drug Development (USA) [1] stated an increase of the total capitalized costs of 8,5% per year (regardless of price inflation) with a consequent decreases in success rates. According to Marshall and Rowan, alternative methods can be a solution to find new treatments at lower costs and without the ethically questionable use of animal testing. In particular, organs-on-chip represent an innovative method that could favor new discoveries in health research like specified by Zhang & al [2]. Different micromodels have already been elaborated for muscles, bones, brain and more specifically blood brain barrier, gut, liver, as well as multi-organs systems, so it only follows that a lung-on-chip would be developped.
It could be extremely interesting to build a human-on-chip (see Fig. 1) that will model the interactions between different organs, but it is also essential to develop simulations of tissue-tissue interfaces and more generally of local organ behavior. Fundamental exchanges happen by ways of the respiration process, especially on the capillary-alveolar interface. Being able to reproduce lung properties on a micro-device will help to better understand its functions and can also allow to simulate pulmonary diseases.
Mouse models already to partially reproduce pulmonary injuries already exist, but microfluidic devices like organ-on-chips can model the mechanical and physiological responses of an organ or more specifically of a tissue-tissue interface exclusively. Moreover, access is easier in the case of a microchip model than for a living mouse. Lungs-on-chip could allow a more precise control of the cellular micro-environment in a way closer to the in vivo biochemical context than the other in vitro simulations.
Challenges in the reproduction of pulmonary thrombosis in a lung-on-chip
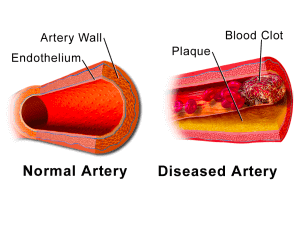
Huh & al. [3] used the organ-on-chip principles to represent the alveolar-capillary interface. Indeed, the alveolar-capillary gas exchanges are essential to the lung function. Being able to reproduce this lung unit can be helpful for nanotoxicology studies and disease simulations. According to Jain & al. [4] pulmonary thrombosis is a major cause of mortality in lung diseases like in ALI (acute lung injury). A blood clot (see Fig. 2) forms locally in a pulmonary vessel and can cause a respiratory failure due to the lack of blood flow in a part of the lung.
Research is ongoing to find proper models of thrombus formation in lung vessels with the aim of developing new therapeutic drugs targeting the inflammatory mechanisms underlying thrombi formation. However, the many animal models built to represent the formation of microvascular thrombosis in lungs are limited because they could not be exactly similar to the human lungs. Besides, experimenting on animals is under ethics debate. Research should therefore evolve toward efficient in vitro models. Jain & al. prospect the hypothesis that organs-on-chips can better represent the thrombosis mechanisms than the existing artificial models. Among other advantages, it allows easier reconfiguration and access thanks to its separate compartments.
Technical characteristics of the microdevice
Alveolar representation
The Wyss Institute develops several pulmonary microchips [3]–[5]. Huh & al. [3] grew both alveolar epithelial and endothelial cells on each side of a PDMS (polydimethylsiloxane) membrane covered with an extracellular matrix (ECM) (see Fig. 3). In vivo, the ECM provides structural support and segregates tissues, the model should thus integrate them for inter-cellular communication and to avoid direct contact between cells of interest and the silicone wall. To reproduce at best the alveoli, the epithelium cells were in contact with air whereas the endothelial cells were in contact with a fluid mirroring blood properties. Two lateral chambers were also added to simulate the pressure changes in the alveoli. Applying vacuum to these chambers causes a deformation of the separating membrane and therefore models the expansion-contraction of the alveolus wall due to the physiological breathing movements.
More on Lung-on-chip systems:

- Lung-on-a-Chip: Origins and Development
- Comparison between organ-on-chip, standard in vitro and in vivo tests
- A short overview of Lung-on-Chip systems – the technology and the potential use in human medicine
- Air-liquid interface and optimized cell culture substrate for a microfluidic lung-on-chip application
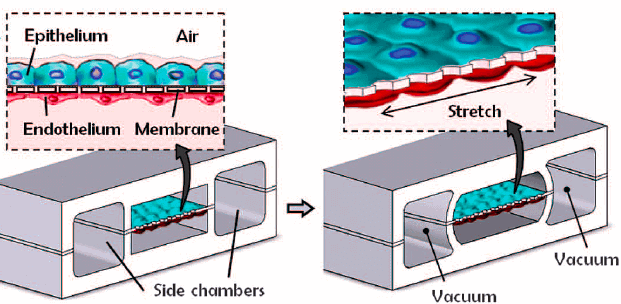
Figure 3: Taken from D. Huh, B. D. Matthews, A. Mammoto, M. Montoya-Zavala, H. Y. Hsin, and D. E. Ingber, “Reconstituting Organ-Level Lung Functions on a Chip,” Science, vol. 328, no. 5986, pp. 1662–1668, Jun. 2010
Pulmonary thrombosis model
Based on previous works on lung-on-a-chip microdevices [3] [5], the Wyss laboratory could elaborate an innovating alveolus-on-chip microdevice reproducing a pulmonary thrombosis. They modified the system described before by using primary human lung cells instead of culture cells. They increased the chambers dimensions to have more exposed area. Human vascular endothelial cells from umbilical cord (HUVEC) were also added all over the walls of the bottom chamber to be able to replace the fluid mimicking plasma with real human blood (see Fig. 4). In fact, in vivo, blood is not directly in contact with the extracellular matrix.

Real blood or “ersatz”?
In the microdevice developed by Jain & al., whole blood in native state was used. Substitutes are often used instead of real blood because of technical or practical difficulties due to blood natural tendency to clot. Human cell blood medium can be used to mimics the principal blood flow characteristics. For example, Li & al. [11] choose to use a cell culture medium with fetal bovine serum for their research on microvessels’ functionalities. However, the medium can only imitate blood properties. It can be an interesting approximation for some simulations but thrombosis is a blood disease! It seems better to precisely consider all the rheologic properties of the blood.
Recalcified citrated or fresh native whole blood?
In the case studied, whole blood was first citrated to avoid excess of coagulation and then recalcified. Citrated whole blood can be perfused longer than fresh whole blood without clotting. Rajwal & al. [12] found comparable parameters for both types of native state whole blood and approved a possible use of citrated blood in clinical evaluation of coagulation states.
[ooc_rebound]
Lung-on-chip findings
Pulmonary thrombus formation process
Jain & al. [4] from the Wyss Institute first noticed that coating the four walls with ECM in the alveolus-on-a-chip, or lung-on-chip model avoid platelet adhesion to the walls and thrombi formation. This microdevice can thus adequately represent a healthy pulmonary vessel behavior. To simulate an intravascular thrombosis, the TNF-α (Tumor necrosis factor) was added to the upper chamber. It is an inflammation-involved cytokine that recruits leukocytes and activates platelets, which triggers thrombi formation [6]. It was measured by Jain & al. that the permeability of lung vessels increases proportionally to the TNF-α concentration. They also measured a raise of ICAM-1 concentration on the endothelium chamber, below which follow by thrombi formation on the endothelial membrane. An in vitro model of endothelial thrombosis formation was therefore obtained by releasing TNF-α in the upper compartment.
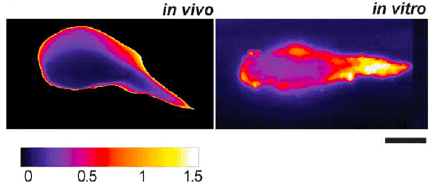
Prof. Ingber laboratory team [4] observed a similar shape and binding dynamic for the thrombosis model-on-a-chip compared to the in vivo laser-induced thrombi formation in a mouse model. The new model established on a microchip also demonstrates another point generally observed in vivo but never seen previously in vitro: the intra-thrombus variations due to a central kernel surrounded by a more unstable region (see Fig. 5).
To better demonstrate the potentiality of lung-on-chip for research, Jain & al [4] tried to add LPS (lipopolysaccharides) to the lung-on-chip. LPS are endotoxins present on the outer membrane of Gram-negative bacteria. These large molecules are often used to induce pulmonary vascular injury because it promotes leukocytes recruitment [7] [8]. At the tissue level represented by the presence of only the vascular endothelium, no thrombosis was observed. A contrario, at the organ-level simulated by a chip with both the epithelial and endothelial cells, intravascular platelets aggregates are observed. The gap areas between endothelial cells increase after the LPS treatment. Jain & al. [4] also found an increase of three specific cytokines following the LPS adding: IL-6 (interleukin), IL-8 and monocyte chemotactic-protein. They noticed similar physiological reactions in vivo: it is possible to increase the induction of lung vascular thrombosis by injecting LPS when the vessels are laser-injured.
Globally, the Wyss Institute demonstrated, using an alveolar microchip, that LPS-induced thrombosis is correlated with an inflammation process mediated by cytokines and induced by interactions between alveolar epithelial cells and vascular endothelial cells.
Using the alveolus-on-a-chip to evaluate a potential antithrombotic treatment
Once they assessed the lung alveolus-chip as a proper model for thrombosis formation, they used it to test possible drug treatments. They choose to study the effects of PM-2 (Parmodulin-2) that have been shown in both in vivo and in vitro models to improve vascular fluidity and thus decrease the risk of thrombosis formation. Aisiku & al. [9] distinguished parmodulins, a family of PAR1 (Protease-activated receptor 1) antagonists, and compared them with others antagonists. They noticed that parmodulins reduce vascular inflammation without causing endothelial injury. Based on previous studies, Jain & al. decided to analyze the action of PM-2 in their alveolus chip compared to a mouse model. Effects of PM-2 in both models match. Therefore, they demonstrate that their lung alveolus-on-a-chip model could potentially be used for drug testing.
Further possibilities using a lung-on-chip
To conclude, it has been demonstrated that a lung-on-a-chip with alveolus could properly represent the mechanical and physiological reaction of an in vivo alveolus. It allows an interesting real-time visualization of tissue-tissue interface. Moreover, the Wyss Institute [4] was able to integrate human blood flow to the microdevice to produce a model closer to the living processes. They noticed good correlations between their in vitro model and the real clotting dynamics in pulmonary vessels due to inflammations. Some aspects of the model can still be improved on because it does not consider the breathing movement. It was already done for the alveolus-capillary interface model by Huh & al. [3]. The Wyss Institute also used HUVEC cells from umbilical cord whereas lung endothelial cells have some specificities, even if these endothelial cells are highly similar.
However, they could use the alveolus-on-a-chip to assess the therapeutic potentiality of a molecule. It creates opportunities for future drug assays at a lower cost and an extremely higher speed. The door is also open for the modeling of other pulmonary diseases by the way of the microchip techniques. Benam & al. (2015) [10] still used this method to develop a small airway-on-a-chip that they employ to mimic the physiological reactions happening during acute asthmatic crisis. Other pulmonary complications could also be analyzed in the future using this simple and efficient technique. Our lung-on-a-chip model pack illustrates how to perform such experiments in an automated and simple way.
Endothelial cells can be cultured on a chip using the endothelial cell culture beta Pack.
References
- J. A. DiMasi, H. G. Grabowski, and R. W. Hansen, “Innovation in the pharmaceutical industry: New estimates of R&D costs,” J. Health Econ., vol. 47, pp. 20–33, May 2016.
- B. Zhang and M. Radisic, “Organ-on-a-chip devices advance to market,” Lab Chip, vol. 17, no. 14, pp. 2395–2420, 2017.
- D. Huh, B. D. Matthews, A. Mammoto, M. Montoya-Zavala, H. Y. Hsin, and D. E. Ingber, “Reconstituting Organ-Level Lung Functions on a Chip,” Science, vol. 328, no. 5986, pp. 1662–1668, Jun. 2010.
- A. Jain et al., “Primary Human Lung Alveolus-on-a-chip Model of Intravascular Thrombosis for Assessment of Therapeutics,” Clin. Pharmacol. Ther., Jul. 2017.
- D. Huh et al., “A Human Disease Model of Drug Toxicity–Induced Pulmonary Edema in a Lung-on-a-Chip Microdevice,” Sci. Transl. Med., vol. 4, no. 159, p. 159ra147-159ra147, Nov. 2012.
- P. Pignatelli et al., “Tumor necrosis factor-α as trigger of platelet activation in patients with heart failure,” Blood, vol. 106, no. 6, pp. 1992–1994, Sep. 2005.
- M. Uchiba and K. Okajima, “Antithrombin III (AT III) Prevents LPS-Induced Pulmonary Vascular Injury: Novel Biological Activity of AT III,” Semin. Thromb. Hemost., vol. 23, no. 06, pp. 583–590, Dec. 1997.
- K. Murakami et al., “Activated protein C attenuates endotoxin-induced pulmonary vascular injury by inhibiting activated leukocytes in rats,” Blood, vol. 87, no. 2, pp. 642–647, 1996.
- O. Aisiku et al., “Parmodulins inhibit thrombus formation without inducing endothelial injury caused by vorapaxar,” Blood, vol. 125, no. 12, pp. 1976–1985, Mar. 2015.
- K. H. Benam et al., “Small airway-on-a-chip enables analysis of human lung inflammation and drug responses in vitro,” 2015.
- X. Li, S. Xu, P. He, and Y. Liu, “In Vitro Recapitulation of Functional Microvessels for the Study of Endothelial Shear Response, Nitric Oxide and [Ca2+]i,” PLOS ONE, vol. 10, no. 5, p. e0126797, May 2015.
- S. Rajwal, M. Richards, and M. O’Meara, “The use of recalcified citrated whole blood – a pragmatic approach for thromboelastography in children,” Pediatr. Anesth., vol. 14, no. 8, pp. 656–660, Aug. 2004.
- Written by Marjorie Metzger, corrected by Julie Cavallasca, under the supervision of Dr. Guilhem Velve Casquillas
For more information or Technical discussion
Microfluidics knowledge
Do you want tips on how to best set up your microfluidic experiment? Do you need inspiration or a different angle to take on your specific problem? Well, we probably have an application note just for you, feel free to check them out!


 Job
Job Collaborations
Collaborations Customer
Customer Other
Other